Why Do Babies With Downs Syndrome Have Chd
![]() Open access peer-reviewed chapter
Open access peer-reviewed chapter
Congenital Heart Disease in Down Syndrome
Submitted: July 23rd, 2017 Reviewed: September 19th, 2017 Published: Jan 31st, 2018
DOI: 10.5772/intechopen.71060

IntechOpen Downloads
1,887
Total Chapter Downloads on intechopen.com
![]()
Altmetric score
Overall attending for this capacity
![]()
Citations

Abstract
Down syndrome remains the near common chromosomal aberration in live-born infants in the earth today. The association between Down's syndrome and congenital eye disease (CHD) is well known, and information technology is widely recognized that CHD contributes significantly to the morbidity of children with Down syndrome. The reported incidence of CHD in Down's syndrome patients is between 40 and 60%. The near commonly described defect is complete atrioventricular septal defect (AVSD), which comprises 30–40% of all cardiac defects. Complex genetic factors are involved. Routine cardiac screening of all newborn babies with Down's syndrome is recommended. Expert groups suggest that the cardiac condition of all children with Down syndrome should exist established by 6 weeks of age to let appropriate and timely treatment fugitive the establishment of irreversible pulmonary vascular illness that would brand cosmetic surgery incommunicable.
Keywords
- Down syndrome
- built center disease
- screening
- AVSD
- pulmonary hypertension
*Address all correspondence to: cmcmahon992004@yahoo.com
1. Introduction
Down syndrome remains the well-nigh common chromosomal aberration in live-born infants in the world today [1]. The association betwixt Downward syndrome and congenital heart affliction (CHD) is well known. It is widely recognized that CHD contributes significantly to the morbidity and mortality of children with Down syndrome. Despite this there continues to be reports of children with Downwardly syndrome who present with serious CHD too late for the best chance of a adept cardiac outcome [2]. Early recognition of lesions is pivotal to obtain the best possible outcome, and pedagogy is still needed. In this chapter, we discuss the incidence and main types of CHD occurring in the setting of Down syndrome. Nosotros focus mainly on atrioventricular septal defect (AVSD), which accounts for thirty–forty% of all cardiac defects in Down syndrome patients. Nosotros review genetic consideration and as well hash out the principles of surveillance for cardiac affliction in this population.
Advertising
2. Prevalence and genetics
Prevalence of Down's syndrome is estimated to be effectually 1–2 per 1000 live births [one]. The reported incidence of CHD in Down syndrome patients is between twoscore and 60% [1, 2, 3]. The most usually described defect is consummate AVSD which comprises 30–40% of all cardiac defects. The types of CHD described in Downwards syndrome do seem to follow a stock-still pattern; in that location are high numbers of septal defects in general; tetralogy of Fallot is described, merely in that location are lower rates of other conotruncal defects like transposition or conditions such as coarctation [4]. Prevalence of private lesions is given later in Table i.
| Per centum of Downwardly syndrome patients afflicted past report | ||||
|---|---|---|---|---|
| Tubman et al. [3] | Frid et al. [17] | Freeman et al. [8] | Stoll et al. [xviii] | |
| AVSD | 38% | 47% | 39% | thirty% |
| VSD | xv% | 33% | 43% | 22% |
| ASD | 21% | 8% | 42% | 25% |
| Tetralogy of Fallot | — | ii% | six% | 3% |
| Coarctation | — | 1% | — | v% |
| TGA | — | — | — | — |
| Patent ductus | 18% | 9% | — | 5% |
Table ane.
Pct of patients with Down syndrome affected by congenital heart illness by defect.
Obviously the triplication of chromosome 21 suggests that genes located in this surface area are likely to play an of import part in the development of CHD. However the fact that Down syndrome is non invariably accompanied by CHD implies that more than complex genetic factors are involved. No unmarried gene candidate has been identified nonetheless [one]. Recent research implicates Hsa21-encoded genes in the development of CHD [five]. Genes for several matrix-related proteins COL-α1 and COL-α2 and Down's syndrome cell adhesion molecule (DSCM) are located in chromosome 21. Overexpression of these genes for collagen matrix-related proteins has been associated with development of AVSD [four]. Nonetheless not all AVSDs are associated with trisomy 21. Other genes non located on chromosome 21 and environmental factors may play a role [1, 5].
Mutations in the cell adhesion molecule cysteine-rich epidermal growth cistron-like domain (CRELD) 1 on chromosome 3 have too been implicated in the genetics of CHD in Down syndrome and correspond to one of the specific genetic loci identified for AVSD [6]. This molecule is idea to exist essential to the process of cellular adhesion and formation of the endocardial cushions. Overexpression of the junction adhesion molecule (JAM) two has as well been shown to potentiate CHD in mice that already take CRELD1 mutation [7]. Undoubtedly the genetic influence of chromosome 21 on CHD is complex and notwithstanding to be fully understood.
In that location is evidence to suggest that sexual activity and indigenous differences do exist in the incidence of CHD in Downwardly syndrome, particularly among those with AVSD. There is a predominance of female infants affected by AVSD and VSD [8]. Black infants with Down syndrome appear to take effectually twice the risk of AVSD equally white infants, whereas Hispanic infants have a much smaller risk than white infants [eight]. The type of lesion is thought to vary according to geographical area. For example, in Brazil the about frequently described defect is an atrial septal defect (ASD) [9, x]. In Asia the most mutual lesion is a ventricular septal defect (VSD) [11]. A group in Sweden reports AVSD as the well-nigh frequent lesion like other Western European countries and the Us. Interestingly they also note a decreasing frequency of complex CHD in Down syndrome; such a trend could exist explained by selective termination of fetuses with Down syndrome in some areas [12].
Advertising
3. Surveillance and screening
The American University of Pediatrics recommends routine cardiac screening of all newborn babies with Down's syndrome [13]. This argument is echoed by the Down syndrome Medical Involvement group (DSMIG UK). They recommend that the cardiac status of all children with Down's syndrome should be established by half-dozen weeks of age [2]. Age at evaluation is an of import factor for reduction in morbidity and bloodshed rates. Failure to recognize cardiac defects early in life can have serious consequences including institution of irreversible pulmonary vascular disease that makes corrective surgery incommunicable [three]. The fact that children still occasionally present to pediatric cardiology clinics in this fashion indicates that the importance of early detection is non fully best-selling, even in the present era [9, xiv]. Neonatal and infant mortality in patients with Down syndrome remains higher than in the general population, primarily due to CHD [ane].
Clinical exam solitary remains insufficient to reliably diagnose CHD in Down syndrome with merely around 40% of newborns having a cardiovascular abnormality detected based solely on clinical findings [iii, 15]. An ECG is probable to exist abnormal, specially in the setting of AVSD, and an abnormal ECG has been shown to take a high positive predictive value for congenital heart disease [3]. Taken together clinical test and ECG are more powerful than either individually [3].
Echocardiography is undoubtedly the most effective single diagnostic test still fifty-fifty it is not 100% effective in identifying lesions in the neonatal menstruation. Authors acknowledge that echocardiography should merely exist carried out by pediatric cardiologists or experienced pediatricians with special interest in cardiology that have access to the necessary equipment and technical skills [3, 15]. There should be a low threshold for repeating the investigation if symptoms or signs of cardiac disease nowadays at any age, even with a history of previously normal echocardiogram [2]. Diagnosis of purely physiological shunts such a PFO or PDA may cause unnecessary worry for some parents.
The DSMIG advise that all babies with a diagnosis of Down syndrome should have a thorough clinical examination and ECG performed shortly afterwards diagnosis and that the urgency of their cess by a pediatric cardiologist should exist determined on the basis of these investigations, such that those with abnormal signs or aberrant ECG exist seen within 2 weeks for echocardiogram and those felt to be at lower risk based on the initial tests be seen inside half dozen weeks from birth [two].
Advertisement
4. Common cardiac defects occurring in Down syndrome
The major types of congenital heart defect occurring in Down's syndrome are listed in Tabular array ane. Every bit noted earlier the most mutual defect is AVSD, which can affect up to xl% of patients [1]. Conversely around 80% of all AVSDs occur in children with Down syndrome [xvi]. Nosotros describe the morphology and pathophysiology of some of the major types of CHD associated with Downward syndrome.
AVSD, atrioventricular septal defect; VSD, ventricular septal defect; ASD, atrial septal defect; TGA, transposition of the peachy arteries.
4.ane. Atrioventricular septal defect (AVSD)
The term AVSD covers a broad spectrum of CHD characterized by a mutual atrioventricular junction with coexisting deficiency in the atrioventricular septum. AVSD comprises around seven% of all CHD and is also referred to equally an endocardial cushion defect [nineteen].
The common atrioventricular junction is ordinarily ovoid with unwedging of the left ventricular outflow tract from the usual position between mitral and tricuspid valves. Instead of separate inlet valves, the AV junction is guarded by a common valve, which often is comprised of 5 leaflets, two of which are bridging leaflets beyond the crest of the interventricular septum (Figure 1). These are termed superior and inferior bridging leaflets, respectively. There is also a left lateral (mural) leaflet, right anterosuperior leaflet, and a right inferior leaflet [sixteen, xix].

Figure i.
The arrangement of the common atrioventricular valve leaflets in consummate AVSD.
The Rastelli nomenclature from 1966 divides complete AVSD into 3 subgroups on the basis of the beefcake of the superior bridging leaflet and its chordal attachments (Effigy two). In Rastelli type A, the superior bridging leaflet is divided at the level of the ventricular septum; in Rastelli type B, the division of the superior bridging leaflet occurs to a right ventricular papillary muscle; and in Rastelli type C, the superior bridging leaflet is undivided or costless floating. Rastelli type C is the about common arrangement found in Downwards syndrome [twenty].

Figure 2.
Rastelli nomenclature. Type a (pinnacle): The superior bridging leaflet is divided at the ventricular septum. Type B (centre): The division occurs to a correct ventricular papillary muscle. Type C (bottom): The superior bridging leaflet is undivided.
In complete AVSD, shunting occurs at both atrial and ventricular levels; however, attachment of the bridging leaflets to the crest of ventricular septum results in an exclusively atrial shunt through a primum ASD, also called a partial AVSD (come across after), whereas attachment of the bridging leaflet to the atrial septum results in exclusively ventricular shunting (Effigy three).
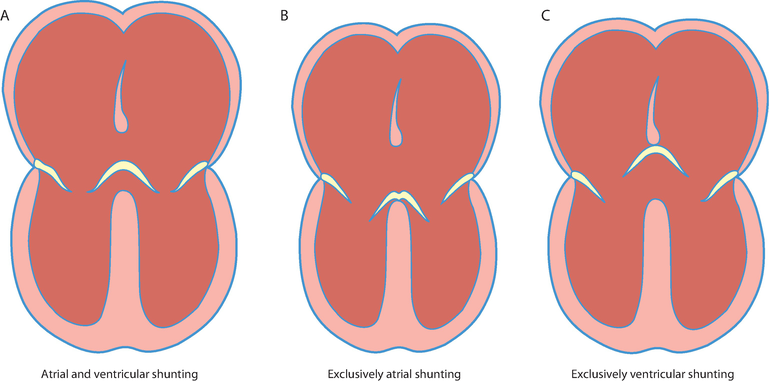
Figure 3.
Resultant shunting in complete AVSD depends on the arrangement of the bridging leaflets with the atrial and ventricular septum. (A) atrial and ventricular shunting, (B) exclusively atrial shunting, (C) exclusively ventricular shunting.
Other congenital heart defects commonly associated with AVSD include left ventricular outflow tract obstacle peculiarly in the setting of a Rastelli blazon A superior bridging leaflet every bit there is extreme unwedging of the aorta from its usual position and consequent elongation of the outflow tract. Ventricular hypoplasia and atrial isomerism are also described although infrequently with Down syndrome. Tetralogy of Fallot is the most commonly observed clan and is seen in up to 6.7% cases of AVSD [20]. There is a high incidence of associated other actress cardiac abnormalities. I study of 87 patients with Tetralogy and AVSD reported that 67% of these patients had Down syndrome [21].
Clinical presentation relates to the morphology of the AVSD and any associated defects. If the ventricular component is large, left to right shunting occurs after the offset few weeks of life as the pulmonary vascular resistance falls, and the babe will develop signs of congestive middle failure. If there is associated significant AV valve regurgitation, ventricular imbalance or coarctation signs of cardiac failure volition occur much before [16, 20]. There is a pocket-size subgroup of patients with complete AVSD who do not develop signs of cardiac failure despite a pregnant ventricular component. In these individuals there is persistent elevation of pulmonary vascular resistance [20].
In the present era, medical handling is aimed at optimizing the patient'due south status to get to corrective surgery. This includes maximizing fluids and calorie intake, oft with supplemental nasogastric tube feeding to promote expert diet. Symptomatic management of congestive eye failure is with diuretics and ACE inhibitor therapy. The aim of surgery is to completely close the septal defects and repair the AV valve. Today surgery is offered to all Down syndrome patients with CHD although this was non always the instance. Surgical results are skilful, and there is believed to be no extra risk from the concomitant presence of Down syndrome [22, 23]. Surgical repair is aimed in the beginning few months of life and certainly earlier 6 months one-time every bit irreversible pulmonary vascular disease is more likely to develop quickly in patients with Down syndrome and AVSD. Surgery is usually successful with depression operative bloodshed. The almost recent statistics from National Found for Cardiovascular Outcomes Research (NICOR) suggest that survival following consummate AVSD repair is 99.5% at xxx days post-op and 91.9% at 1 twelvemonth [24]. Without corrective surgery many patients with complete AVSD will die in infancy, with just 4% surviving beyond 5 years old [25]. Those who survive will develop pulmonary vascular affliction and eventual reversal of the systemic to pulmonary shunt with accompanying cyanosis or Eisenmenger'south syndrome.
Postoperative complications following surgical repair of complete AVSD are listed in Table two. Those seen virtually usually are left ventricular outflow tract obstruction and left AV valve regurgitation. Left AV valve regurgitation forms the most common reason for reoperation in well-nigh surgical series [26]. Interestingly, the morphology of the AV valve well-nigh associated with Down syndrome, Rastelli type C, may actually exist more than favorable for surgical repair as in that location is ofttimes extensive bridging of both superior and inferior bridging leaflets resulting in less left AV valve regurgitation. Surgical series demonstrate that patients with Down's syndrome experience greater freedom from reoperation for left AV valve regurgitation than those without Downwards syndrome [27].
| • Left atrioventricular valve regurgitation |
| • Left ventricular outflow tract obstruction |
| • Late-onset consummate eye block |
| • Pulmonary vascular disease |
| • Atrial or ventricular rhythm problems |
| • Left atrioventricular valve stenosis |
| • Right atrioventricular valve stenosis or regurgitation |
| • Remainder ventricular septal defect |
| • Aortic incompetence |
Table 2.
Long-term complications post-obit repair of consummate AVSD [xvi, xix].
four.2. Primum atrial septal defect/partial AVSD
In an isolated primum ASD or partial AVSD, the AV junction is a common construction; however, there are separate right and left AV valve orifices equally a band of valve tissue joins the superior and inferior bridging leaflets. The AV valves appear at the same level, and there may be regurgitation through the zone of opposition or "cleft" in the left AV valve (Figure iv). Timing of surgery in this case is less crucial especially if at that place is minimal AV valve regurgitation. Repair is often carried out in belatedly infancy or early childhood. Isolated primum ASD unrepaired carries 50% mortality before the age of xx years [16]. Surgical results are good, and 30-mean solar day and ane-year survival are 98.viii and 98.7%, respectively [24]. Long-term complications are similar to those described following AVSD repair with the almost common reason for reoperation being left AV valve regurgitation followed past left ventricular outflow tract obstacle [26].

Figure iv.
Organization of the common atrioventricular valve leaflets in primum ASD.
4.3. Tetralogy of Fallot
Tetralogy of Fallot is a conotruncal defect caused by the anterior and cephalad deviation of the infundibular septum, which leads to the development of the four characteristic components: ventricular septal defect, overriding aorta, correct ventricular outflow tract obstruction, and right ventricular hypertrophy (Figure 5). Tetralogy of Fallot occurs in around half dozen% of patients with Down syndrome and is the most common cyanotic heart defect to nowadays in this patient group. Conversely effectually 8% of patients with Tetralogy of Fallot have Downwards syndrome, although this is slightly higher in fetal serial [28].
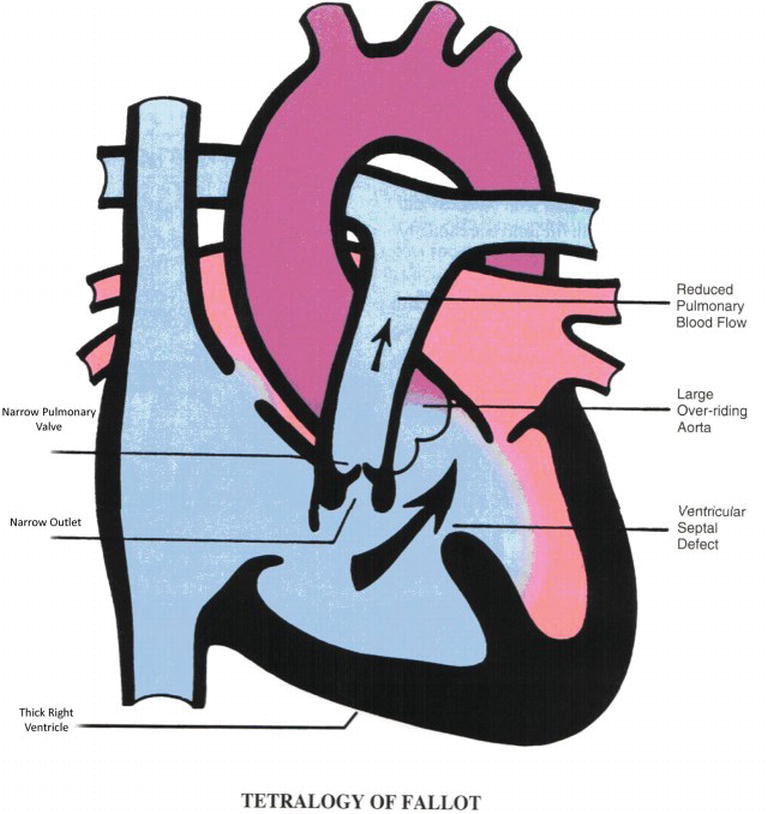
Figure v.
Diagrammatic representation of tetralogy of Fallot.
Clinical presentation of tetralogy of Fallot depends very much on the degree of outflow tract obstruction nowadays. Patients may present with profound central cyanosis in the neonatal menstruum if the obstruction is astringent and may actually be duct dependent, i.e., at that place is insufficient pulmonary blood period in one case the ductus arteriosus closes. These patients require palliation with a Blalock-Taussig shunt or ductal stent to secure pulmonary blood menses and allow growth for corrective surgery. If there is trivial outflow tract obstacle, the patient may exhibit signs and symptoms of congestive cardiac failure equally in that location volition be a big left to right shunt through the VSD; in this instance in that location volition be piffling or no cyanosis.
Most ordinarily, patients fall somewhere in between and have a degree of outflow tract obstruction often presenting with an ejection systolic murmur and some cyanosis [28]. The degree of cyanosis is oftentimes variable, and patients may have cyanotic spells, which result from an acute increase in right to left shunting due to spasm of the muscular infundibular region. Patients with cyanosis or frequent spells that cannot be managed with beta blocker therapy may require a RVOT stent. Cosmetic surgery is performed at around 6–eight months of age. Outcomes are good, and survival following tetralogy repair is 99.7% at 30 days and 97.8% at 1 year [24]. Mutual long-term complications are listed in Table iii.
| • Pulmonary regurgitation |
| • Correct ventricular dilatation and dysfunction |
| • Residual right ventricular outflow tract obstruction |
| • Branch pulmonary stenosis |
| • Rhythm problems |
| • Aortic incompetence |
| • Aortic root dilatation |
Table 3.
Long-term complications following tetralogy of Fallot repair [29].
The relief of correct ventricular outflow tract obstacle during tetralogy of Fallot repair results in chronic pulmonary regurgitation, which subsequently leads to right ventricular dilatation necessitating interventions. The well-nigh frequent reason for reoperation in this patient group is to replace the pulmonary valve either surgically or percutaneously [28, 29]. There is show to suggest that patients with Downward syndrome who accept undergone tetralogy of Fallot repair come to pulmonary valve replacement more than often than patients without Down's syndrome. This is felt to be due to the presence of pulmonary arterial hypertension, likewise mutual in Down's syndrome, which contributes to more than severe pulmonary regurgitation and earlier RV dilatation [30].
4.4. Ventricular septal defect (VSD)
A ventricular septal defect is defined every bit a hole between the right and left ventricles. In most series it is the second most mutual form of CHD described in Down syndrome (Table 1). VSDs are generally classified depending on what portion of the ventricular septum they span, illustrated in Figure six. In Down syndrome VSDs often occur in the inlet septum [31]. In a large series of patients with Downwardly syndrome, inlet VSD was one of the most frequently reported subtypes. Muscular and subarterial VSDs were not described [32]. Inlet VSD is associated with abnormalities of the left AV valve with straddling chordal and papillary muscle attachments [31]. In the setting of Down syndrome, these defects probable grade function of the AVSD complex described earlier [32].

Effigy 6.
Diagrammatic representation of possible VSD locations on standard echo views. (A) long axis view, (B) short axis view at aortic valve level, (C) short axis view through ventricles, (D) iv bedroom view, (E) left ventricular outflow tract view.
Similarly to AVSD, a VSD results in a left to right shunt with extra pulmonary blood flow, the magnitude of which depends on both the size of the defect and the patient's pulmonary vascular resistance. Hemodynamically significant defects are repaired before 6 months of historic period. Similar AVSD uncorrected lesions will pb to the development of pulmonary vascular disease and Eisenmenger'southward syndrome [31].
four.v. Other lesions
From tardily adolescence there is evidence of an increased incidence of asymptomatic mitral valve prolapse (MVP) and aortic incompetence in children with Down syndrome. These are often asymptomatic; notwithstanding, the MVP in particular can progress to symptomatic mitral regurgitation, and it is recommended that auscultation continues to be part of surveillance for individuals with Down's syndrome in adult life [ii].
Advertizing
5. Pulmonary hypertension in Down syndrome
Patients with Down's syndrome are considered to be at higher risk of pulmonary arterial hypertension both with and without CHD. This is probable to be multifactorial, just the high incidence of CHD and airway problems undoubtedly plays a pivotal office in its development [33]. Down's syndrome patients have a high incidence of gastroesophageal reflux with micro-aspiration, recurrent respiratory infections, and sleep apnea. They may experience chronic hypoxia from upper airway obstruction in the class of tracheobronchomalacia, stenosis, or subglottic compromise [33]. There is a high prevalence of persistent pulmonary hypertension of the newborn in infants with Down syndrome, and equally discussed earlier, at that place is a small subset of Down's syndrome CHD patients who proceed to have elevated pulmonary vascular resistance across the newborn menses [xvi].
In the setting of a significant left to right shunt, intrinsic lung abnormalities such every bit abnormal pulmonary arterioles, a smaller number of alveoli, and impaired endothelial function contribute to the evolution of pulmonary arterial hypertension in association with CHD [34]. Every bit observed earlier, timely corrective surgery will forbid irreversible lung damage and development of Eisenmenger's syndrome. Despite this move to early on surgery, there remain a significant number of Down syndrome patients with Eisenmenger's syndrome among the adult built heart disease population. Some studies estimate that as many as 50% of the total population of Eisenmenger's patients have Down syndrome; in that location is too evidence to propose that this group receives significantly less therapy and is often under-managed [35].
Advertisement
6. Conclusions
Congenital heart affliction is one of the most frequent associations with Downwardly syndrome and remains a major cause of morbidity and mortality among patients. Over half of Down's syndrome patients accept CHD the about mutual form existence consummate AVSD. Ethnic and geographical variations amongst lesions take been described. Early recognition of lesions is paramount to permit appropriate and timely treatment. To this end, cardiac screening should be undertaken in all newborn infants with Down syndrome.
References
- one.
Vis JC, MGJ D, Winter MM, et al. Down syndrome: A cardiovascular perspective. Journal of Intellectual Disability Research. 2009; 53 :419-425 - 2.
DSMIG United kingdom of great britain and northern ireland. Guidelines for Sssential Medical Surveillance for People with Down Syndrome. 2007. Available form: http://dsmig.org.uk/library/manufactures/guideline-cardiac-5.pdf . [Accessed: Baronial 31, 2017] - three.
Tubman TRJ, Shields MD, Craig BG, et al. Congenital centre illness in Down's syndrome: Ii year prospective early on screening study. British Medical Journal. 1991; 302 :1425-1427 - 4.
Colvin KL, Yeager ME. What people with Down's syndrome tin teach us about cardiopulmonary disease. European Respiratory Review. 2017; 26 :160098 - v.
Asim A, Kumar A, Muthuswamy Due south, et al. Down syndrome: An insight of the disease. Journal of Biomedical Scientific discipline. 2015; 22 :41 - six.
Priestly MD, H2o J, Maliszewska C, et al. Detailed mapping of a congenital heart disease cistron in chromosome 3p25. Journal of Medical Genetics. 2000; 37 :581-587 - seven.
Li H, Edie S, Klinedinst D, et al. Penetrance of congenital middle affliction in a mouse model of Down syndrome depends on a trisomic potentiator of a disomic modifier. Genetics. 2016; 203 :763-770 - 8.
Freeman SB, Edible bean LH, Allen EG, et al. Ethnicity, sexual activity and the incidence of congenital heart defects: A report from the national Down syndrome project. Genetics in Medicine. 2008; 10 :173-180 - 9.
Mourato FA, Villachan LRR, de Silva Mattos Due south. Prevalence and profile of built heart illness and pulmonary hypertension in Down syndrome in a pediatric cardiology service. The Revista Paulista de Pediatria 2014; 32 :159-163 - 10.
Bermudez BEBV, Medeiros SL, Bermudez MB, et al. Down's syndrome: Prevalence and distribution of congenital heart disease in Brazil. São Paulo Medical Periodical. 2015; 133 :621-624 - 11.
Jacobs EG, Leung MP, Karlberg J. Distribution of symptomatic built heart disease in Hong Kong. Pediatric Cardiology. 2000; 21 :148-157 - 12.
Bergstrom Southward, Carr H, Ptereson Thou, et al. Trends in built heart defects in infants with Down's syndrome. Pediatrics. 2016; 138 :e20160123 - xiii.
American University of Pediatrics. Health supervision for children with Down syndrome. American Academy of Pediatrics. 2001; 107 :442-449 - 14.
Dennis J, Archer N, Ellis J, et al. Recognising heart illness in children with Down syndrome. Athenaeum of Disease in Babyhood – Education and Practice. 2010; 95 :98-104 - 15.
Wren C, Richmond S, Donaldson L, et al. Presentation of congenital center illness in infancy: Implications for routine exam. Archives of Disease in Childhood. Fetal and Neonatal Edition. 1999; 80 :F49-F53 - 16.
Craig B. Atrioventricular septal defect: From fetus to adult. Middle. 2006; 92 :1879-1885 - 17.
Frid C, Drott P, Lundell B, et al. Mortality in Down's syndrome in relation to congenital malformations. Journal of Intellectual Disability Research. 1999; 43 :234-241 - 18.
Stoll C, Dott B, Alembik Y, et al. Associated congenital anomalies amid cases with Down syndrome. European Periodical of Medical Genetics. 2015; 58 :674-680 - 19.
Calkoen EE, Hazekamp MGG, Blom NA, et al. Atrioventricular septal defect: From embryonic development to long term follow upwardly. International Journal of Cardiology. 2016; 202 :784-795 - 20.
Cohen MS. Common atrioventricular canal defects. In: Lai WW, Mertens LL, Cohen MS, Geva T, editors. Echocardiography in Pediatrics and Congenital Centre Disease: From Fetus to Developed. United kingdom of great britain and northern ireland: Wiley-Blackwell Publishing; 2009 - 21.
Vergara P, Digilio MC, Zorzi AD, et al. Genetic heterogeneity and phenotypic anomalies in children with atrioventricular canal defect and tetralogy of Fallot. Clinical Dysmorphology. 2006; 15 :65-70 - 22.
Rizzoli Thou, Mazzucco A, Maizza F, et al. Does Down syndrome affect prognosis of surgically managed atrioventricular canal defects? The Journal of Thoracic and Cardiovascular Surgery. 1992; 105 :945-953 - 23.
Masuda M, Kado H, Tanoue Y, et al. Does Downwards syndrome affect the longterm results of complete atrioventricular septal defect when the defect is repaired during the first year of life? European Journal of Cardio-Thoracic Surgery. 2005; 27 :405-409 - 24.
NICOR website. Bachelor from: https://nicor4.nicor.org.uk/CHD/an_paeds.nsf/vwContent/dwelling house . [Accessed: Aug 27, 2017] - 25.
Berger TJ, Blackstone EH, Kirklin JW, et al. Survival and probability of cure with and without functioning in complete atrioventricular canal. The Annals of Thoracic Surgery. 1979; 27 :104-111 - 26.
Najim HK, Coles JG, Endo M et al. Complete atrioventricular septal defects: results of repair, adventure factors and freedom from reoperation. Apportionment. 1997; 96 :II-311-315 - 27.
El-Najdawi EK, Driscoll DJ, Puga FJ, et al. Operation for partial atrioventricular septal defect: A forty year review. The Periodical of Thoracic and Cardiovascular Surgery. 2000; 199 :880-890 - 28.
Srivastava S, Parness IA. Tetralogy of Fallot. In: Lai WW, Mertens LL, Cohen MS, Geva T, editors. Echocardiography in Pediatrics and Congenital Heart Disease: From Fetus to Adult. United Kingdom: Wiley-Blackwell Publishing; 2009 - 29.
Downing TE, Kim YY. Tetralogy of Fallot: General principles of management. Cardiology Clinics. 2015; 33 :531-541 - 30.
Sullivan RT, Frommelt PC, Hill GD. Before pulmonary valve replacement in Downwardly syndrome patients following tetralogy of Fallot repair. Pediatric Cardiology. 2017; 38 :1251-1256 - 31.
Forbus GA, Shirali GS. Anomalies of the ventricular septum. In: Lai WW, Mertens LL,Cohen MS, Geva T, editors. Echocardiography in Pediatrics and Congenital Middle Disease: From Fetus to Adult. U.k.: Wiley-Blackwell Publishing; 2009 - 32.
Marino B, Papa Grand, Guccione P, et al. Ventricular septal defects in Down syndrome. Anatomic types and associated malformations. American Periodical of Diseases of Children. 1990; 144 :544-545 - 33.
D'Alto M, Mahadevan VS. Pulmonary arterial hypertension associated with congenital heart disesase. European Respiratory Review. 2012; 21 :328-337 - 34.
Cappelli-Bigazzi M, Santoro G, Battaglia C, et al. Endothelial cell part in patients with Down syndrome. The American Periodical of Cardiology. 2004; 94 :392-395 - 35.
Van de Bruaene A, Delcroix Grand, Pasuet A, et al. The Belgian Eisenmenger syndrome registry: Implications for treatment strategies? Acta Cardiologica. 2009; 64 :447-453
Submitted: July 23rd, 2017 Reviewed: September 19th, 2017 Published: January 31st, 2018
© 2018 The Author(south). Licensee IntechOpen. This affiliate is distributed under the terms of the Creative Commons Attribution 3.0 License, which permits unrestricted employ, distribution, and reproduction in whatsoever medium, provided the original work is properly cited.
Source: https://www.intechopen.com/chapters/57288
0 Response to "Why Do Babies With Downs Syndrome Have Chd"
Post a Comment